

Inside MA-PD Premium Trends
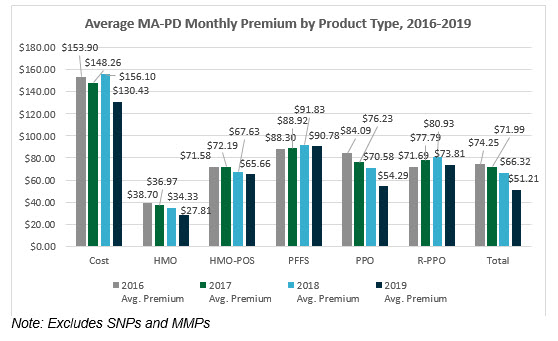
With the release of the 2019 landscape files, benefit information and Star Ratings data, now is the time to update your market analyses to understand trends in your current and potential markets. Nationwide, 2019 monthly premiums for Medicare Advantage Prescription Drug Plans (MA-PDs), excluding Special Needs Plans (SNPs) and Medicare-Medicaid Plans (MMPs), range from $0 per month to $388 per month, with the average monthly premium being $51.21. The average monthly premium of MA-PDs decreased from 2018 by 23%. While a decrease aligns with the overall premium trends since 2016, this level of decrease is unprecedented. The overall decrease in the 2019 average monthly premium is nearly four times the average premium decrease seen in 2018 (8% decrease) and seven times the average premium decrease seen in 2017 (3% decrease). Since 2016, MA-PDs have seen an overall decrease in monthly premium amounts by 31%, from $74.25 to $51.21 – a $23 decrease. How have premiums changed in your market(s)?
As discussed often in recent years, $0 monthly premium plans are on the rise. Notably, nearly half (44%) of MA-PDs have a $0 monthly premium. This segment saw the most growth in the distinct number of plan benefit packages (PBPs) offered with an increase in nearly 300 new $0 MA-PDs. The premium segment that saw the second most growth in the distinct count of PBPs from 2018 to 2019 is MA-PDs, with a monthly premium between $1 and $50; 28% of MA-PDs fall in this premium range, with an increase of nearly 121 PBPs. Additionally, the number of PBPs available with a monthly premium over $150 has decreased since 2016. Gorman Health Group (GHG) expects to see these trends continue.
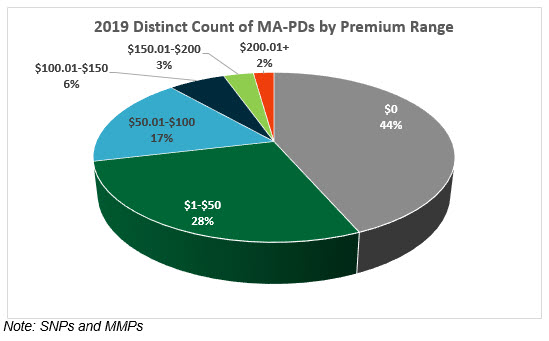
While 44% of all PBPs are $0 monthly premium plans, over half (56%) of all Health Maintenance Organizations (HMOs) are $0 premium plans, and 75% of $0 premium plans are HMOs. We expect to see the number of $0 PBPs to continue to increase, especially in the HMO product. Remarkably, nearly 30% of Preferred Provider Organization (PPO) products are $0 premium plans. For 2019, there are an additional 124 $0 premium plan PPOs available. This is nearly three times the overall $0 PPO growth in 2018. With the growth in availability of $0 PBPs, Medicare Advantage Organizations (MAOs) will need to continue to push for innovative product design benefits to remain competitive. Even $0 premium plans need to explore creative ways to make their plans stand out in the $0 crowd.
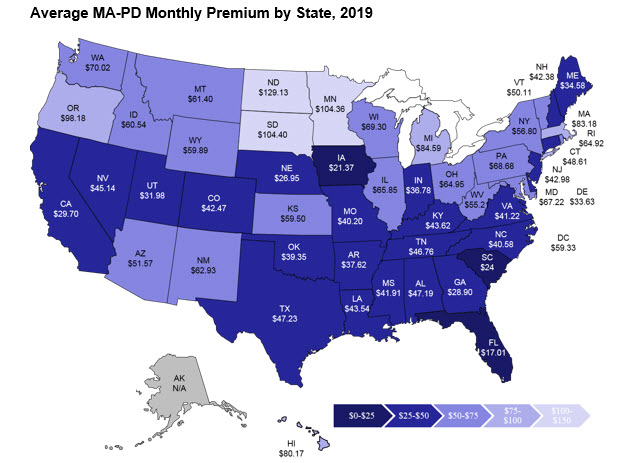
The average monthly premium by state (excluding Puerto Rico and territories) ranges from $129 in North Dakota ($129.13) to $17 in Florida ($17.01). As in years prior, the states with the highest average premium are found in the plains states region – North Dakota ($129.13), South Dakota ($104.40), and Minnesota ($104.36). This is not surprising as these states continue to have large enrollment in Cost plans, which are traditionally structured to have high premiums. For example, in 2019, the average monthly premium of Cost plans is $130.43.
So what does this all mean for you? Now is the time to replicate a similar analysis to understand your current and/or potential markets. Additionally, assess the key benefits offered, including ALL supplemental benefits. Some of these benefits include the maximum out-of-pocket, inpatient hospital cost sharing, primary care physician and specialist cost sharing, and supplemental benefits like routine dental, vision, and hearing – and don’t forget to assess plans offering targeted supplemental benefits. How do your plans stack up to the competition? Are you growth goals for this coming Annual Election Period (AEP) realistic? Are your AEP marketing and sales strategies ready to face the competition and meet growth goals – what can you adjust? What must you consider for 2020? No, it’s not too early to start planning – product and benefit development is a year-long process.
Resources:
Stay connected to industry news and gain perspective on how to navigate the latest issues through GHG’s weekly newsletter. Subscribe
Learn how a single platform designed specifically for Medicare can streamline enrollment and offer a better way to deliver a return on your plan’s investment. Click here

The 2019 Star Ratings Are Out!
The 2019 Star Ratings are out! While our experts crunch the numbers and analyze the data, here are a few “fast facts:”
Of the 360 contracts rated in both 2018 and 2019,
- 80 earned higher overall ratings in 2019 compared to 2018
- 90 earned lower overall ratings in 2019 than in 2018
- 190 maintained the same rating in 2018 and 2019
The more things change, the more they stay the same.
- 45% of Medicare Advantage Prescription Drug Plans (MA-PDs) (170 contracts) earned 4+ stars in 2019, compared to 44% (170 contracts) in 2018
- Approximately 74% of MA-PD enrollees are currently in contracts that will have 4+ stars in 2019, compared to 73% in 2018
- The 2019 average Star Rating (weighted by enrollment) is 4.05 in 2019, compared to 4.07 in 2018
- 376 contracts met the criteria to receive an overall rating in 2019, compared to 385 in 2018
- Humana (with 84% of its 3.5 million members in 4+ star contracts), United (with 70% of its 5.4 million members in 4+ star contracts), and Kaiser (with 100% of its members in 4+ star contracts) continue to dominate the competitive Medicare Advantage (MA) Star Ratings arena
Sponsors with the most members impacted by year-over-year changes in the overall ratings are among industry giants:
- Some of the big winners in 2019 include Cigna, Highmark, MCS, Wellcare, and Centene
- Among those with the most members in contracts earning lower ratings in 2019 are United, Anthem, and Blue Cross and Blue Shield of Minnesota
Although the Star Ratings headwinds are strong for new plans, sponsors continue flocking to MA:
- 22% of contracts operating less than 5 years earned 4+ Star Ratings in 2019, compared to 41% of contracts operating between 5 and 10 years, and 54% of contracts operating more than 10 years
- 210 contracts were not rated in 2019 because they were too new to receive a rating or did not have enough data to be rated, compared to 168 in 2018
See a trend in the Star Ratings you’d like us to comment on in our upcoming Star Ratings webinar? Get in touch with one of our experts, and we’ll address it in our webinar!
Resources:
Stay connected to industry news and gain perspective on how to navigate the latest issues through GHG’s weekly newsletter. Subscribe

The CMS Fall Conference Highlights
The Centers for Medicare & Medicaid Services (CMS) annual fall conference never misses in providing important information for Sponsors. This year’s conference was held in Baltimore on September 6, 2018. Conference materials can be found on the Compliance Training, Education & Outreach website here. CMS covered many areas, but here I’m focusing on two key areas of the conference: Medicare Communications and Marketing Guidelines (MCMG) updates and appeals and grievances classification best practices.
MCMG
One of the most important clarifying statements from CMS was definitively communicating the MCMG replaces the Medicare Marketing Guidelines (MMG) and any guidance within it. What does that mean? If previous MMG guidance is not dictated in the MCMG, Sponsors should consider that guidance obsolete. While many had assumed that was the case, it’s always better to get clarity straight from the source. This single statement should resolve many looming questions by Sponsors.
Of equal significance was CMS further outlining the meaning of “marketing” material. In order to be considered “marketing,” the material must meet both intent and content requirements. If only one of these distinctions is met, the material would not be considered “marketing.” The example used to help drive this message was the Evidence of Coverage (EOC). The EOC has content that would meet “marketing” definitions, however, the intent is not to persuade a beneficiary to enroll, so it is considered a communication. This new guidance will eliminate much burden for Sponsors in relation to the number of materials requiring CMS review and submission. While this removes some administrative burden, the oversight may need to be more stringent as health plans are now even more responsible for correct classification of documents and ensuring documents still comply with all CMS requirements. Additionally, documents must be available upon request.
Other noteworthy clarifications from CMS:
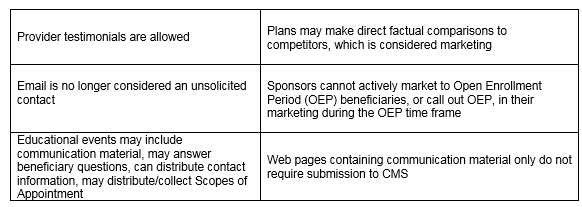
An updated MCMG was distributed by CMS on September 6, 2018.
APPEALS & GRIEVANCES
In their continued effort to help Sponsors in the appeal and grievance space, CMS and Sponsor representatives presented classification best practices. CMS reminded Sponsors of key words when classifying appeals and grievances:
Inquiry ----- a question
Grievances ----- a dissatisfaction
Coverage/Organization Determination ----- a decision to provide or pay
Appeal ----- a dispute of a previous decision
Several health plan speakers shared their best practices. Some of the valuable recommendations that changed their organization included:
- Centralized Customer Service staff focused on identifying appeals and grievances. Staff training focused on real-life examples and involved frequent refreshers.
- Cross-functional all staff on grievances, coverage and organization determinations, and appeals. Training not only included correct identification and classification but also the downstream member and CMS impact of failure to correctly identify complaints. This holistic approach supports the member experience and greater CMS compliance.
- Intake staff who review cases quickly to identify any potential misclassification of cases. Root cause analysis as a routine part of processing. So often the focus is on resolving the identified issue for that member, which is critical. Equal importance is remedying any systemic concerns to prevent the problem from impacting other members. The presenters discussed how root cause was discussed in routine meetings with other departments for brainstorming and resolution.
- Embedded Compliance staff within the business units. A great trend in the industry in recent years is to have an operational Compliance person located in critical operations units. They are available to help staff work through complex issues where a keen eye on regulatory guidance is needed. This keeps cases moving forward and allows staff to feel supported all while maintaining high compliance.
CMS conferences have always been valuable resources in clarifying new changes or functions that have the attention of CMS. Don’t miss utilizing this valuable resource to stay current.
 Gorman Health Group provides training tools, conducts mock audits, and supports process improvement initiatives related to Parts C & D appeals and grievances? We also provide interim staff for clients when they have a need in this area.
Gorman Health Group provides training tools, conducts mock audits, and supports process improvement initiatives related to Parts C & D appeals and grievances? We also provide interim staff for clients when they have a need in this area.
Resources:
Stay connected to industry news and gain perspective on how to navigate the latest issues through GHG’s weekly newsletter. Subscribe





